


Featured Post
Who Can Own a Medical Spa?

AmSpa Events
Med spa technology is advancing quickly. Electronic medical records, EMR, customer relationship management, CRM, lead management systems, LMS, automated marketing ...

Clinical
By Belmar Pharma SolutionsYour bustling, successful practice is full of women who really care about their appearance, and they trust ...

AmSpa Events
Regenerative medicine is becoming the new center of medical spa wellness services. Patients are asking about longevity, peptides, exosomes, hormonal ...

Business
By XiteAs the medical aesthetics industry continues to mature, many medical spa owners are beginning to think seriously about retirement ...


Marketing
By AestheticsPro For medical spa owners looking to reach their clients in the most...
Top Tags
January 24, 2023
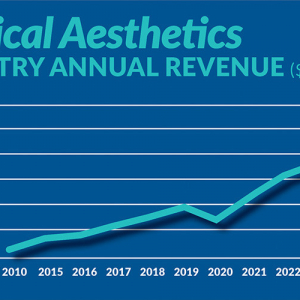
Figure displays medical aesthetics industry annual revenue ($ in billions). By Madilyn Moeller Day-to-day life...

February 24, 2021
By Bradford E. Adatto, Partner, ByrdAdattoIntravenous (IV) therapy has been used to provide nutrition and...

September 21, 2023
By Patrick O'Brien, JD, General Counsel, American Med Spa Association [AmSpa first published a...

July 19, 2023
By Patrick O'Brien, General Counsel, American Med Spa Association (AmSpa) UPDATE #2 (2/08/2024): Since...